The current Ebola emergency may not present a direct threat to the UK public but if, or when, a similar disease does break out on these shores we need to be sure that our front-line workers have the protection they need.
5000 kilometres. That's the distance between London and Freetown which is the capital of Sierra Leone and one of the countries at the heart of the current Ebola outbreak in West Africa.
To the mind's eye, West Africa might be another continent, another world even, but in reality it's just seven hours away in the serene comfort of an airliner seat. The truth is that diseases that once took months or years to spread widely can now be transmitted globally in the space of a few hours. With over 50 million transcontinental air passengers passing in and out of the UK every year (1) and a growing global trade in agricultural products the risk of deadly and difficult to control diseases arriving on these shores is very real and growing.
And the threat is not just from globalisation. With the emergence of drug-resistant bacteria ('superbugs') and as complex new viral infections continue to surface, it is getting harder and harder to suppress and control even relatively 'common' pathogens such as salmonella and streptococcus (2). Although the antibiotic wonder drugs that have appeared over the past 70 or so years have had a dramatic impact on the treatment of infectious diseases, bacteria that resist antibiotics are now widespread. And the uncanny ability of bacteria and viruses to mutate over time has led to the emergence of new infectious diseases at a rate of about one every year since the 1970s (3) with many of these being both highly contagious and resistant to antibiotics. According to the World Health Organisation dangerous pathogens such as bacteria, viruses and parasites are responsible for over 16% of the annual deaths worldwide (4). And it is estimated that drug-resistant strains of bacteria are already responsible for 5,000 deaths a year in the UK and 25,000 deaths a year in Europe (5).
Omnipresent
Bio-hazards can present themselves in numerous ways and their very omnipresence can make them very difficult to manage and control. A bio-hazard may be bacterial, viral, parasitic or fungal and source materials, such as contaminated body fluids, tainted packaging and dirty work surfaces are all potential bio-risks. Causal origins of biological hazards range from decaying foodstuffs and faecal bacteria to highly virulent medical wastes, germ warfare agents and zoonosis (animal transfer). All of these bio-hazards and many others relate to the presence of infectious biological agents and biologically-derived toxins or contaminated materials including organic dusts and mould spores.
Bio-hazards also have widely varying transfer mechanisms. Some infectious diseases, influenza for example, can be contracted directly by touch or by inhaling respiratory droplets while others, such as tuberculosis, are mainly spread by airborne transmission. Malaria, on the other hand is transmitted by mosquitoes whilst Ebola and AIDS generally require the direct transfer of infected body fluids.
The need for protective procedures and barriers
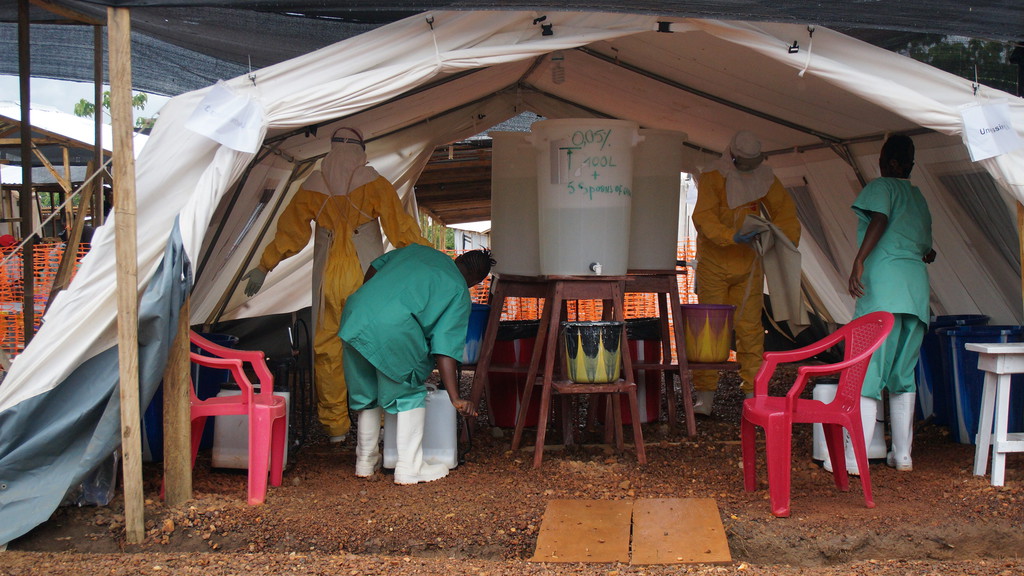
In practice, things are never so clear cut. Ebola, for example, can survive and remain infectious for several days outside the human body (7) so it can be contracted simply by contact with a contaminated surface. And this means that stretchers, ambulances, medical equipment and PPE need to be rigorously decontaminated in the event of any possible exposure. Keeping these areas clean to the standard necessary to contain highly virulent pathogens such as Ebola is a challenge in itself and requires money, education and commitment. Such measures would no doubt put the emergency services under considerable strain should Ebola or a similar disease gain a foothold in the UK.
As can be seen from the recent Ebola outbreaks, exposure to biological contaminants can have very serious and rapidly escalating health consequences which means there is little room for complacency or delay when it comes to putting the correct protective procedures in place. Cases of paramedics and first responders contracting infectious diseases from patients and then passing them on, are not unknown (8). We must be prepared to invest in better public-health surveillance as well as better training, education and biological protection of health workers, emergency responders and support personnel.
The vast number of potentially dangerous micro-organisms and the huge range of possible biological risk conditions means that the selection of personal protection equipment (PPE) for personnel faced with live threatening pathogens can be a very complex exercise indeed. In addition to effective body protection against naturally spreading infections and diseases, there is a need for personal protection in emergency response scenarios whenever biological agents are being manufactured, handled, distributed, studied, administered, neutered, removed or disposed of. The types of sites where these activities can occur include hospital facilities, defence and military establishments, medical and biological research laboratories and biotechnology production facilities. Bio-hazard precautions are also necessary in a wide range of crisis scenarios from flood management operations to trauma scene cleaning to bio-terrorism responses.
Seeking guidance
In all cases of biological hazard exposure a dedicated risk assessment must be carried out on all PPE ideally with reference to the performance classes described in European Standard EN 14126 (9). Biological agents are classified into four categories (10) and, due to the extremely wide compass of risk involved with infective agents, it is absolutely essential that expert guidance is sought when selecting appropriate PPE for the different levels of hazard.
And safety for emergency responders isn't just about having the right protective gear. The correct training is every bit as important. It is a fact that many cases of biological hazard exposure have been due to lapses of attention or procedure; things that can easily happen in the stressful conditions of an emergency response situation. Armand Sprecher, the medical adviser to Doctors Without Borders for haemorrhagic fevers, affirmed this in a recent interview for NPR in the United States (11): "Where we see health care worker infections when the PPE is in place, [the worker] did something to override the PPE: they didn't wear it appropriately or contaminated their hands in the process of getting [the suit] off."
A matter of time
In recent years we have seen MERS, SARS and Ebola all take the stage as untreatable diseases and so far they have been successfully contained. But it's an uphill fight. In many people's eyes it is only a matter of time before another major international medical emergency occurs involving an incurable or very difficult to treat disease. Ebola may not be perceived in some quarters as a huge threat to the UK (12) but it is surely a timely wake up call. The truth is there may be even more threatening diseases just round the corner. The question is: are we ready?
(1) DoT Transport Statistics 2013
(2) Centers for Disease Control and Prevention
(3) World Health Organisation: World Health Report 2007
(4) World Health Organisation: The Global Burden of Disease: 2004 Update
(5) see http://www.bbc.co.uk/news/health-28098838
(6) WHO Disease Outbreak News 8th August 2014
(7) Public Health Agency of Canada; Ebola Virus - Pathogen Safety Data Sheet
(8) Putting their lives on the line: Meningitis in first responders; B. McKenna, Wired 11.18.10
(9) 'Performance Requirements and Test Methods for Protective Clothing Against Infective Agents'
(10) Refs: United States Centers for Disease Control and Prevention (CDC) and EU Directive 2000/54/EC
(11) This Suit Keeps Ebola Out - So How Can A Health Worker Catch It?; M. Silver; NPR; July 24, 2014
(12) "Ebola virus threat to the UK is 'very low"; NHS Choices July 31, 2014